




Contents
Scroll to:
https://doi.org/10.23947/2687-1653-2023-23-3-307-316
Scroll to:
Introduction. Perianal fistula rapidly develops an abscess, requiring surgical decompression. However, simple cases must be managed. However, for patients with renal insufficiency, MRI with contrast is contraindicated. It is proposed to use diffusion-weighted images that can diagnose anal fistulae, showing areas of high signal intensity (inflammatory tissues). The aim is to determine sensitivity of diffusion-weighted image combined with T2 turbo inversion recovery magnitude and as an alternative technique to contrast-enhanced MRI using clinical examination as a reference.
Materials and Methods. Study included fifty patients with a clinical diagnosis of perianal fistula. MRI sequences were T2 turbo inversion recovery magnitude in oblique coronal and axial planes, diffusion-weighted image, and T1 weighted image turbo spin echo (fat suppression) pre- and post-administration of contrast agents in oblique axial planes. Three radiologists evaluated the MR imaging data using a questionnaire of parameters that necessitated a binary response, “yes” or “no” answer.
Results. Diffusion-weighted image combined with axial T2 turbo inversion recovery magnitude sequence had 96.7 %. All raters agreed that it is sensitive enough to correctly identify perianal fistula with a moderate Kappa agreement (k = 0.586) and p-value<0.001. The mean value of rater's responses was 76.7 % represents sensitivity of diffusion-weighted images + T2 turbo inversion recovery magnitude as an alternative technique to T1-enhanced contrast with moderate (k = 0.553) agreement between raters and P-value<0.001.
Discussion and Conclusion. Diffusion-weighted images and T2 turbo inversion recovery magnitude sequences exhibit comparable efficacy to T1-enhanced contrast sequences in detecting perianal fistula. This may be an option for patients with renal impairment who cannot receive an MRI contrast.
Baqir N.F., Ahmed R.S., Mohsen Kh.I. Sensitivity of Diffusion-Weighted Image Combined with T2 Turbo Inversion Recovery Magnitude Sequence and as an Alternative to Contrast-Enhanced MRI in the Detection of Perianal Fistula. Advanced Engineering Research (Rostov-on-Don). 2023;23(3):307-316. https://doi.org/10.23947/2687-1653-2023-23-3-307-316
Introduction. Perianal fistula is a rare condition that is difficult to treat and is associated with patient morbidity. It is the connection between the mucosal lining of the anal canal and the perianal epidermis [1]. The rate of occurrence is approximately two times higher in males than in females. The male-female ratio is 2:1. Perianal discharge that comes and goes, itchiness, discomfort, fever, and localized pain are the most typical symptoms [2]. Perianal fistula is associated with the rapid development of an abscess, necessitating timely surgical intervention for decompression. Consequently, the management of uncomplicated cases is crucial [3]. The treatment of anal fistula involves the excision of the primary fistula opening, any associated tracts, and any supplementary openings while ensuring the preservation of continence [4]. This requires accurate identification of the fistula's internal opening and any secondary abscesses or extensions. Imaging techniques, including magnetic resonance imaging (MRI), are increasingly important in perianal fistula diagnosis [5][6] because they provide the most precise and reliable data regarding the anatomical characteristics of the fistula tract and its association with the anal sphincter muscles. Providing these specific details by MRI has enhanced surgical success rates and reduced the likelihood of recurrence in perianal fistulas [7][8]. T2-weighted with fat suppression (Turbo spin echo or turbo inversion recovery magnitude) MRI is very good at showing a fistula track. Still, some reports have pointed out how hard it is to distinguish between real abscesses that need to be drained by surgery and inflamed masses that cannot be drained and need anti-inflammatory medicine. Gadolinium chelate-enhanced T1-weighted MR scans are often used as a tool to help solve problems [9][10]. Post-contrast MR imaging is the optimal sequence for detecting and characterizing perianal fistula. It is considered the gold standard by various institutions [5][11].
Nonetheless, using gadolinium contrast agents increases expenses and duration and poses a risk of nephrogenic systemic fibrosis in patients already experiencing renal insufficiency. In addition, several studies have found evidence of gadolinium accumulation in the brain's deep nuclei after repeated contrast agent injections [1][12][13]. In recent years, Diffusion-Weighted Imaging (DWI) has provided high differentiation between pathological lesions, such as cancer or inflammatory processes, and the adjacent normal tissue [14]. DWI is a technique that captures variations in water mobility resulting from interactions with macromolecules, cell membranes, and changes in the tissue environment. Therefore, inflammatory tissues may also demonstrate limited diffusivity, resulting in the appearance of high signal areas on DWI, which takes advantage of this property. This sequence has the potential to be helpful in the diagnosis of anal fistulae [15][16].
Moreover, Diffusion-Weighted Imaging can be integrated into customary Magnetic Resonance Imaging (MRI) scans of the perianal fistula, as it removes the need for a contrast agent, has shorter sequence duration, and does not necessitate additional equipment. The diffusion-weighted imaging technique has a naturally low spatial resolution, one of the method's drawbacks. Therefore, the T2 turbo inversion recovery magnitude (TIRM) sequence was added to DWI to assess the perianal fistula to overcome these drawbacks [16][17]. In the T2 TIRM imaging technique, the fistulous tracts are commonly visualized as highly intense linear structures [18]. Additionally, it should be noted that pus, fluid, and granulation tissue manifest as areas of high signal intensity against a background of low signal intensity fat [6][19].
Boruah et al. [20] evaluated the efficacy of diffusion-weighted magnetic resonance imaging (MRI) as a diagnostic tool for perianal fistulae. The study consisted of 47 participants diagnosed with perianal fistula. The MRI results were correlated with the clinical evaluation or the surgical findings. The performance of DWI alone was inferior to that of T2W imaging. Nevertheless, the most notable outcome was the assessment of combined DWI-T2W images, despite the lack of statistical significance compared to DWI or T2W images individually.
Gu et al. [21] explored an alternative technique comparable to Gadolinium-contrast enhancement to assess any morphological changes in the preoperative evaluation of anal fistulas. The study comprised 46 individuals who had received a diagnosis of anal fistula. The gold standard for comparison will involve outcomes derived from surgical pathology. The utilization of FS T2-weighted and diffusion-weighted imaging exhibited similar effectiveness when compared to FS T1-weighted contrast-enhanced imaging for evaluating changes in the morphology of anal fistulas.
This study aims to determine the sensitivity of diffusion-weighted images combined with T2 turbo inversion recovery magnitude (TIRM) and as an alternative technique to contrast-enhanced MRI using the clinical examination as a gold standard reference.
Patients and Methods. The study was carried out between December 2022 and May 2023 at the MRI department of the oncology teaching hospital located in Medical City, Baghdad, Iraq. The research was carried out as a cross-section and utilized a non-randomized design. After a thorough clinical evaluation of each patient, the surgical outpatient clinics sent fifty patients who were thought to have perianal fistulas to the MRI department. Each participant gave their informed written agreement, and the institution's ethical committee gave its stamp of approval before the study was carried out.
The inclusion criteria for this study include adult patients, regardless of gender, who have been diagnosed with a perianal fistula during a clinical examination and have been referred from outpatient surgical clinics.
The exclusion criteria for this study include individuals who fall into specific categories, namely children, pregnant women, and patients who are contraindicated for MRI examinations. This includes patients with cardiac pacemakers or metallic shells and those who experience claustrophobia.
The MRI examinations were performed using 1.5 T scanners (Magnetom Aera, Siemens Healthcare, Germany) equipped with a phased-array surface coil comprising 18 channels. There was no requirement for patient preparation before the examination. During the MRI, patients take a supine position on the examination table, with a phased array surface coil positioned over their pelvic region. It is crucial to ensure correct orientation when using magnetic resonance imaging (MRI) for imaging the anal canal. The planning of the images is performed with the assistance of a sagittal T2-weighted localizer that passes through the middle of the patient. The oblique transverse and coronal sections are orthogonally and parallel to the anal sphincter.
The following MRI sequence parameters were utilized for this investigation: T2 TIRM in the coronal oblique plane (TR/TE: 5000/50, slice thickness: 3 mm, flip angle: 140°, interstice gap: 20 %, number of slices: 34, FOV: 390mm, matrix size: 384×288, signal averages: 1, inversion time (TI): 160 s, acquisition time: 2:27 (min: sec)). T2 TIRM performed in the oblique axial plane (TR/TE: 5040/50 ms, slice thickness: 3 mm, interstice gap: 20 %, flip angle: 140°, number of slices: 36, FOV: 380 mm, matrix size: 384×234, signal averages: 1; inversion time (TI): 160 s, acquisition time: 2:02 (min: sec). Single shot echo planar imaging (EPI) imaging (DWI) in an oblique axial plane (TR/TE: 2600/70, FOV: 380 mm, distance factor: 20 %, slice thickness: 3 mm number of slices: 30, matrix size: 128×128, b-value 50–400–800 with signal averages of 1 for 50, 3 for 400, and 800, acquisition time: 2:22 (min: sec)). And T1 FS TSE in an oblique axial plane before and after administration of contrast agent (TR/TE: 619/20, slice thickness: 3 mm, number of slices: 27, interstice gap: 20 %, flip angle: 160°, FOV: 239 mm, signal averages: 1, matrix size: 192×163, acquisition time: 1:55 (min: sec)).
Three radiologists, each with an advanced radio diagnosis degree and over five years of experience in MRI reporting, were carefully selected for employment at the oncology teaching hospital based on their superior rankings among other radiologists. Furthermore, these individuals consistently produce a substantial volume of over 40 reports per week. They were provided information regarding the patient's clinical suspicion of perianal fistula while unaware of the surgical and prior MRI reports. The radiologists reviewed the MR imaging data sets using a questionnaire of parameters requiring a binary response (yes or no) as follows:
The data were inputted, categorized, and examined using the SPSS (statistical package for social sciences) software program version 26. The data were presented using frequencies and percentages. A significance level of 0.05 or lower was used to determine statistical significance. The study employed the Fleiss kappa test to evaluate the reliability and inter-rater agreement among multiple raters.
Results. The findings of this study were derived from the analysis of a sample of fifty individuals who presented with a perianal fistula as determined through clinical assessment. Most individuals diagnosed with anal fistula were male, comprising 82 % of the cases, while females constituted the remaining 18 % as shown in Figure 1. The mean age of the entire patient population was 39.80 years, and the standard deviation was 12.46 years.
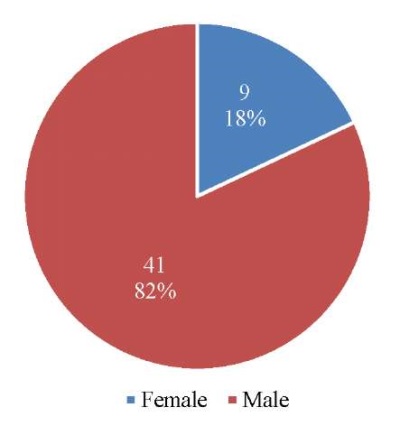
Fig. 1. Frequency distribution of the gender for the 50 participant patients
According to the prepared questionnaire, the three rater's responses about the best visualization of perianal fistula by diffusion-weighted image combined with T2 TIRM and as an alternative method to T1 enhanced contrast. The frequency distribution of the three raters is demonstrated in Table 1. The three raters' responses according to the constructed questionnaire; regarding the best visualization of the perianal fistula compared to the positive clinical examination (standard reference) is represented in Fig. 2.
Table 1
Frequency and percentage of DWI+T2 TIRM and DWI
as an alternative to T1 enhanced contrast images for three raters
|
DWI+T2 TIRM freq. (%) |
DWI image as an alternative to T1 enhanced contrast freq. (%) |
|
|
Rater 1 |
47(94 %) |
37(74 %) |
|
Rater 2 |
49(98 %) |
36(72 %) |
|
Rater 3 |
49(98 %) |
42(84 %) |
|
Total |
50 (100 %) |
|
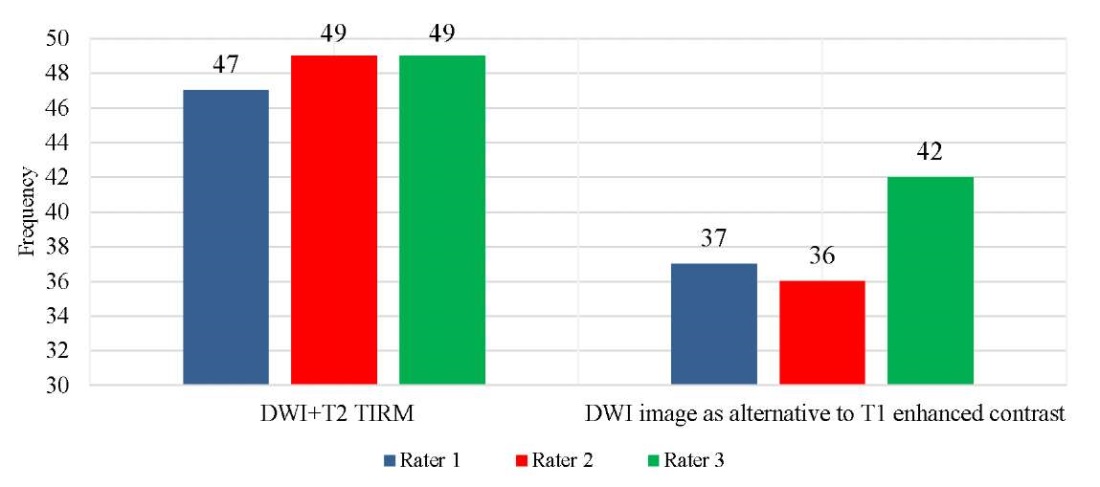
Fig. 2. Bar chart frequency distribution of the raters' opinions
about using diffusion-weighted image combined with T2 TIRM
and as an alternative to T1 enhanced contrast in detecting perianal fistula
The average of the three raters for detecting cases of perianal fistula by each reported MRI sequence is demonstrated in Figure 3. It was found that DWI+ axial T2 TIRM had a higher percentage (96.7 %), which corresponded to the sensitivity of this sequence in the detection of true cases of perianal fistula by the three raters. The average of raters' answers for replacing the T1 FS TSE enhanced contrast with DWI in detecting anal fistula was 76.7 % (sensitivity of DWI +T2 TIRM as an alternative technique to T1 enhanced contrast). The inter-rater kappa agreement was performed to test the reliability of the questionnaire used to evaluate MRI sequences obtained for the visualization of 50 patients clinically diagnosed with perianal fistula, as shown in Table 2. A significant (P-value<0.001) moderate (k=0.586) agreement was found for the question related to the use of optimized DWI + T2 TIRM. Also, significant (P-value<0.001) moderate (k=0.553) agreement between raters when asked to use DWI versus T1 enhanced contrast.
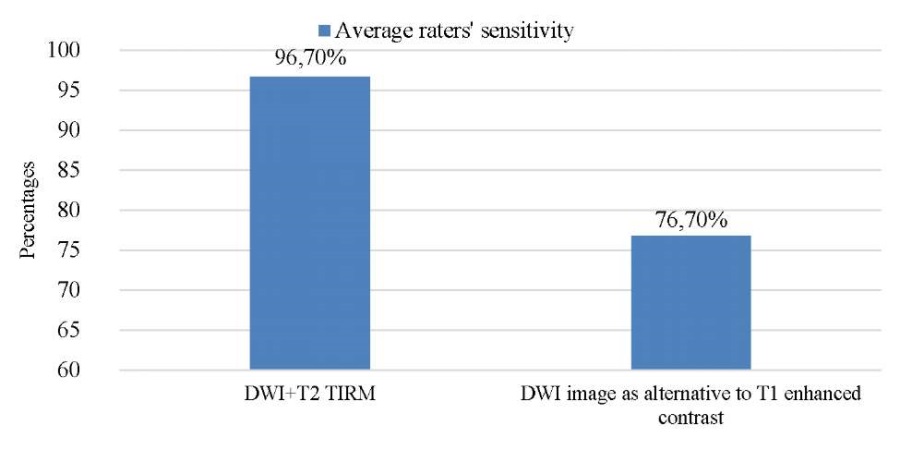
Fig. 3. Bar chart of overall average sensitivity of the raters' opinions (%)
about using different MRI sequences in detecting anal fistula
Table 2
Inter-rater reliability and overall agreement between radiologists
in the diagnosis of anal fistula among 50 patients
|
Sequence used |
Kappa |
95 % CI |
P-value |
|
DWI versus T1 enhanced contrast |
0.553 |
0.548–0.558 |
<0.001 |
|
DWI + T2 TIRM |
0.586 |
0.581–0.591 |
<0.001 |
DWI diffusion-weighted image, TIRM turbo inversion recovery magnitude, CI confident interval.
The presence of a perianal fistula can be seen in a variety of MRI sequences, as shown in Figure 4 and Figure 5, and Figure 6 demonstrates the abscess collection of patients with perianal fistula that shows the well-defined restricted diffusion of the abscess and hyper-signal intensity on T2 TIRM as an alternative technique to T1 enhanced contrast.
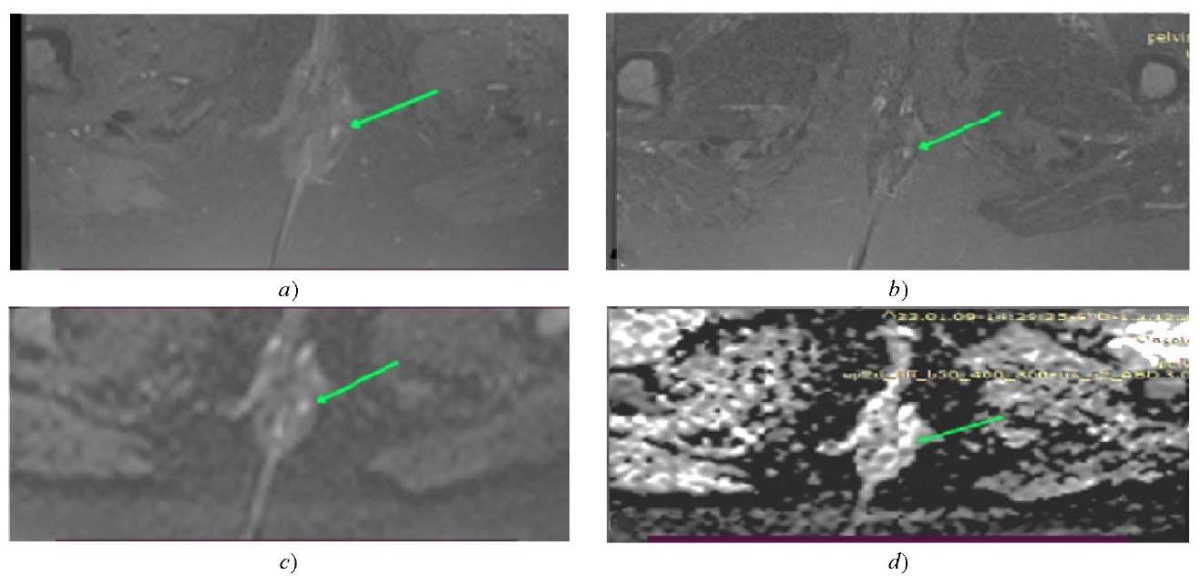
Fig. 4. A 41-year-old female patient presenting
with a left-sided supra sphincteric fistula at 2 o'clock (green arrow);
a — shows the T1 FSTSE enhanced contrast;
b — shows the T2 TIRM;
c — shows the diffusion-weighted image (3 mm slice thickness);
d — shows the ADC map
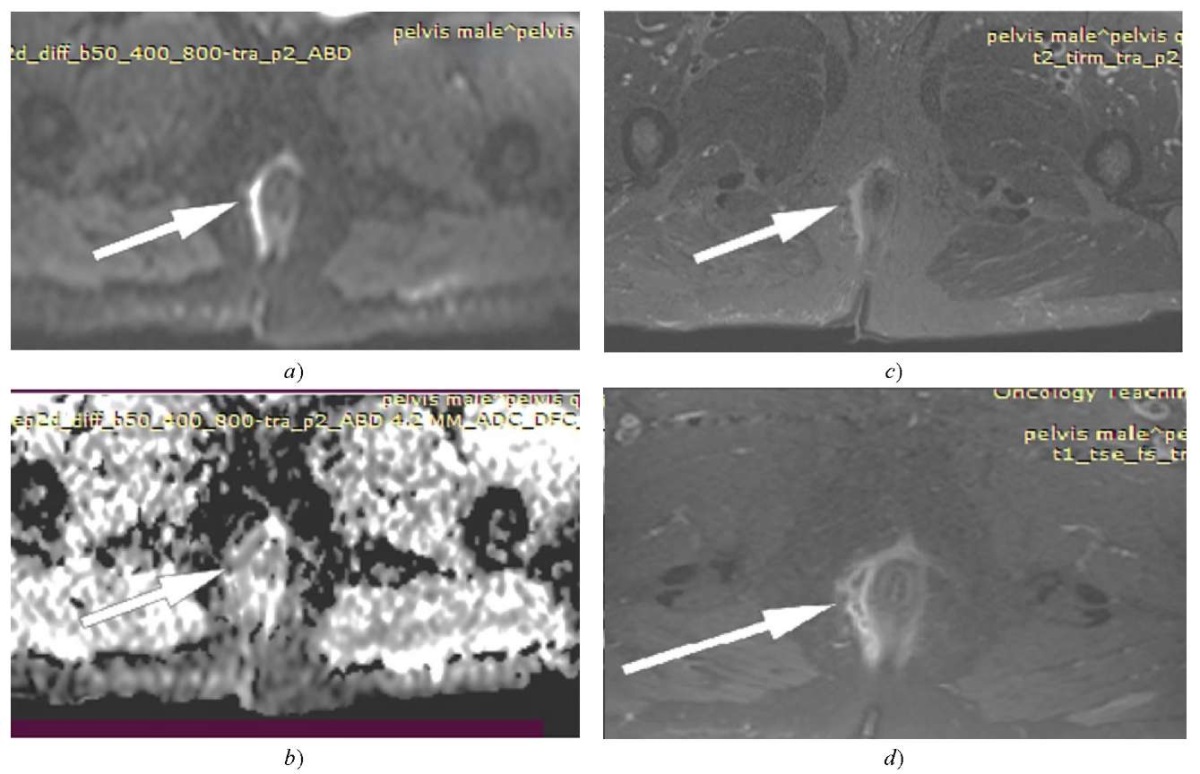
Fig. 5. A 51-year-old male presenting
with a right-sided supra sphincteric branching fistula
with extensive inflammatory changes
and multiple extra sphincteric abscess collections (white arrow),
a — optimized DWI;
b — ADC map shows restrictd diffusion;
c — T2 TIRM shows hyper signal intensity;
d — T1FSTSE post-contrast shows peripheral enhancement.
All the images are in the oblique axial plane
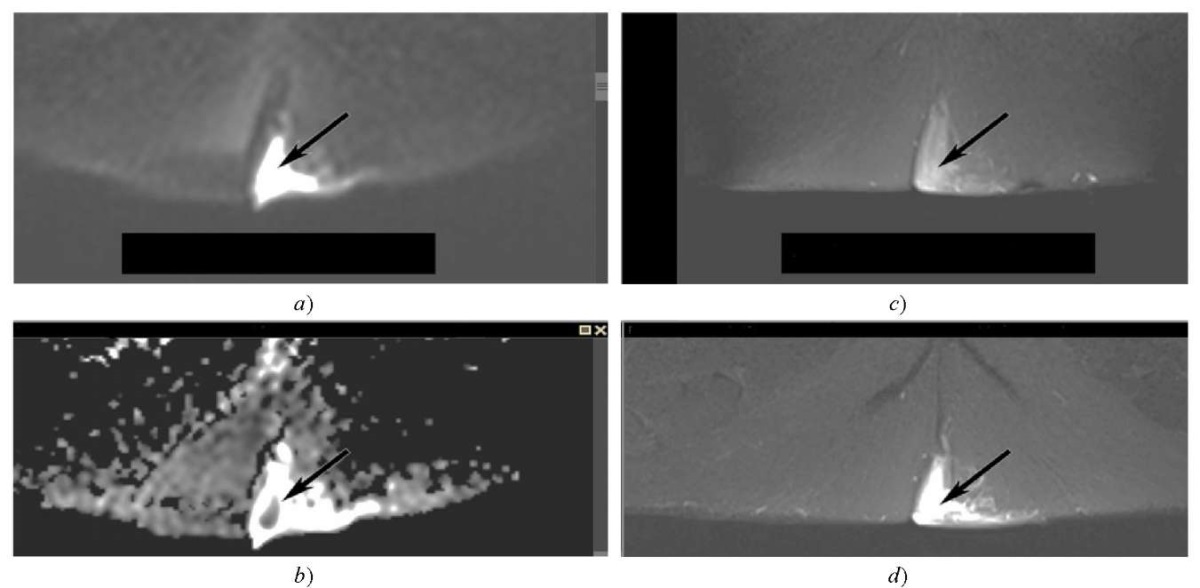
Fig. 6. A 36-year-old male presenting with a left gluteal abscess collection
with surrounding significant soft tissue edema (black arrow),
a — diffusion weighted image;
b — ADC map shows restricted diffusion;
c — T1FSTSE post-contrast shows peripheral enhancement;
d — T2 TIRM shows hyper signal intensity.
All the images are in the oblique axial plane
Discussion. The primary purpose of magnetic resonance imaging (MRI) in the context of perianal fistulas is to establish the extent of the tract, identify any side branches, and determine the presence of deep abscesses, especially at the supra levator level [22]. The utilization of Gadolinium-enhanced T1-weighted images and fat suppression confers distinct advantages in differentiating a fluid-filled tract from an area of inflammation. The wall of the tract displays increased enhancement, whereas the central region exhibits a hypo-intense appearance. Post-contrast gadolinium images exhibit high efficacy in visually representing abscesses [23]. However, the gadolinium contrast agent does have certain limitations. These include an extended duration of magnetic resonance examination, additional costs, the potential deposition of gadolinium contrast in the brain, and contraindications for patients with renal insufficiency (1).
Diffusion-weighted imaging has been proposed as a noteworthy alternative due to its ability to identify inflammatory lesions as areas exhibiting high signal intensity. The fistulous tracks demonstrate increased intensity in diffusion-weighted images, whereas the background signal is significantly attenuated. Consequently, the identification and extent of the fistula can be easily determined [24]. One limitation of diffusion-weighted imaging is its inherent drawback of having a relatively low spatial resolution. Diffusion-weighted imaging was not evaluated as an independent variable in our study. In this study, we evaluated the supplementary benefits of the technique in fat-suppressed T2-weighted imaging, specifically
T2 TIRM (16). In our study, it was observed that all three raters concurred on the suitability of the majority of images derived from the sequences of Diffusion-Weighted Imaging (DWI) combined with T2 Turbo Inversion Recovery Magnitude (TIRM) to delineate anal fistula. Both rater two and rater three reported a percentage of 98, while rater 1 reported a slightly lower percentage of 94 for the images. Hence, the DWI+T2 TIRM sequence exhibited the highest percentage (96.7 %), aligning with the sensitivity of DWI combined with T2 TIRM compared to the clinical examination as the gold standard. The inter-rater kappa agreement was moderate (k = 0.586), with a significant P-value of less than 0.001. It is agreed Fahmy et al. (5) that is conducted a study that revealed a sensitivity of 92.12 % for the detection of perianal fistula when using a combination of diffusion-weighted imaging (DWI) and T2-weighted imaging (T2WI).
However, they regarded T1-weighted imaging (T1WI) post-contrast as the reference standard for comparison. Additionally, Mohsen and Osman [25] evaluated the combined utilization of diffusion-weighted imaging (DWI) and T2-weighted (T2W) sequences to obtain optimal outcomes. The perianal fistulas and abscesses were accurately diagnosed in 97.8 per cent of cases using T2-weighted imaging (T2WI) and T1-weighted imaging post-contrast (T1WI post-contrast) as the established benchmark. Regarding the sensitivity of DWI combined with T2TIRM as an alternative technique to T1 FS TSE post-contrast, our research revealed that rater 3 said that it is sensitive for 42 (84 %), followed by rater one and rater two in the same order, who reported 74 % and 72 % of the sensitivity, respectively. Therefore, an average raters' sensitivity of 76.7 %; there was a significant (P-value 0.001 fair (k=0.370) agreement between the three raters in selecting DWI as an alternative to post-contrast sequence for the detection of perianal fistula. Therefore, it reflects the capability of DWI in clearly delineating perianal fistula, making it comparable to contrast enhancement MRI in the detection of perianal fistula and possibly making it superior to contrast enhancement MRI in the detection of perianal fistula by reducing the amount of time an MRI examination takes and by reducing the adverse effects of contrast agents, particularly in patients with renal impairment. Our findings agree with those of Hori et al. (16), who established that there was not a statistically significant difference (p-value less than 0.05) in the sensitivity between combined contrast-enhanced sequences with T2WI and DWI coupled with T2WI. Also, according to the findings of Fahmy and Dawoud (5), the utilization of a combination of diffusion-weighted imaging (DWI) and turbo inversion recovery magnitude (TIRM) is deemed equivalent to the utilization of post-contrast images in the detection of primary and complicated fistula. The application of Diffusion-Weighted Imaging (DWI) has demonstrated its utility in differentiating between abscesses and inflammatory reactions and assessing the extent of disease activity. Active granulation tissue will exhibit enhancement on post-contrast T1-weighted imaging compared to the fluid in the fistula. Rim enhancement indicates an abscess, while diffuse enhancement is typical of granulation tissue (5). In comparison, diffusion-weighted imaging is a technique that depicts changes in the mobility of water molecules caused by their interactions with cell membranes, macromolecules, and environmental changes in the tissue. On diffusion-weighted imaging (DWI), inflammatory tissues may exhibit reduced diffusivity, resulting in hyper-intense signal regions [26]. The apparent diffusion coefficient (ADC) values observed in abscesses are estimated to be lower than those in healthy tissues. As reported in the scientific literature, this is due to pus, which inhibits the unrestricted diffusion of water molecules (9). As inflammatory tissues typically demonstrate enhanced signal intensity, diffusion-weighted imaging may hold promise as a diagnostic sequence for anal fistulas (6).
Our study has the limitation of not making a quantitative comparison by calculating ADC values in the diffusion-weighted images to diagnose active and inactive perianal fistula compared with the T1 enhanced contrast because of the overloaded work in the institution where the study was conducted. Therefore, we recommend future research to evaluate the ADC value of diffusion-weighted images to diagnose active and inactive perianal fistula compared with the T1 enhanced contrast with a larger sample size.
Conclusion. The sensitivity of diffusion-weighted images in conjunction with T2 turbo inversion recovery magnitude (TIRM) sequences demonstrates a similar level of effectiveness as T1 enhanced contrast sequences in identifying and assessing perianal fistula. This combination of imaging techniques may serve as a viable alternative, particularly for individuals with renal impairment who are contraindicated to administer MRI contrast agents.
1. Cattapan K, Chulroek T, Kordbacheh H, Wancharoenrung D, Harisinghani M. Contrast-vs. Non-Contrast Enhanced MR Data Sets for Characterization of Perianal Fistulas. Abdominal Radiology. 2019;44:446–455. https://doi.org/10.1007/s00261-018-1761-3
2. Gurung G. 3T MR Imaging Evaluation of Perianal Fistulas: an Initial Experience in Nepal. Journal of Society of Surgeons of Nepal. 2016;19(1):25–30. URL: https://api.semanticscholar.org/CorpusID:199464071 (accessed: 10.04.2023).
3. Singh K, Singh N, Thukral C, Singh KP, Bhalla V. Magnetic Resonance Imaging (MRI) Evaluation of Perianal Fistulae with Surgical Correlation. Journal of Clinical and Diagnostic Research (JCDR). 2014;8(6):RC01–04. https://doi.org/10.7860/JCDR/2014/7328.4417
4. Kee Ho Song. New Techniques for Treating an Anal Fistula. Journal of the Korean Society of Coloproctology. 2012;28(1):7–12. https://doi.org/10.3393/jksc.2012.28.1.7
5. Fahmy DM, Dawoud MG. Value of Diffusion Weighted MRI in Assessment of Simple and Complicated Perianal Fistula. The Egyptian Journal of Radiology and Nuclear Medicine. 2017;48(3):553–562. https://doi.org/10.1016/j.ejrnm.2017.03.010
6. Jaime de Miguel Criado, Laura Garcia del Salto, Patricia Fraga Rivas, Luis Felipe Aguilera del Hoyo, Leticia Gutiérrez Velasco, M Isabel Diez Pérez de las Vacas, et al. MR Imaging Evaluation of Perianal Fistulas: Spectrum of Imaging Features. RadioGraphics. 2012;32(1):175–194. https://doi.org/10.1148/rg.321115040
7. Akyel NG, Akın K, Kösehan D, Köktener A. Perianal Fistula Imaging: A Comparison between Two-Channel Superficial Flex Coil and Eight-Channel Body Coil. Polish Journal of Radiology. 2019;84:e430–e435. https://doi.org/10.5114/pjr.2019.89906
8. Omer HK, Jalab HA, Hasan AM, Tawfiq NE (eds.) Combination of Local Binary Pattern and Face Geometric Features for Gender Classification from Face Images. In: Proc. 9th IEEE International Conference on Control System, Computing and Engineering (ICCSCE). New York City, NY: IEEE; 2019. https://doi.org/10.1109/ICCSCE47578.2019.9068593
9. Dohan A, Eveno C, Oprea R, Pautrat K, Placé V, Pocard M, et al. Diffusion-Weighted MR Imaging for the Diagnosis of Abscess Complicating Fistula-in-ano: Preliminary Experience. European Radiology. 2014;24:2906–2915. https://doi.org/10.1007/s00330-014-3302-y
10. Hasan AM, Meziane F, Aspin R, Jalab HA (eds.) MRI brain scan classification using novel 3-D statistical features. In: Proceedings of the Second International Conference on Internet of things, Data and Cloud Computing. New York, NY: ACM; 2017. P. 1–5. https://doi.org/10.1145/3018896.3036381
11. Jiyeon Baik, Seung Ho Kim, Yedaun Lee, Jung-Hee Yoon. Comparison of T2-weighted Imaging, Diffusion-Weighted Imaging and Contrast-Enhanced T1-weighted MR Imaging for Evaluating Perianal Fistulas. Clinical Imaging. 2017;44:16–21. https://doi.org/10.1016/j.clinimag.2017.03.019
12. Marckmann P, Skov L, Rossen K, Dupont A, Damholt MB, Heaf JG, et al. Nephrogenic Systemic Fibrosis: Suspected Causative Role of Gadodiamide Used for Contrast-Enhanced Magnetic Resonance Imaging. Journal of the American Society of Nephrology. 2006;17(9):2359–2362. https://doi.org/10.1681/ASN.2006060601
13. Cansu A, Bekircavusoglu S, Oguz S, Bulut E, Fidan S. Can Diffusion Weighted Imaging Be Used as an Alternative to Contrast-Enhanced Imaging on Magnetic Resonance Enterography for the Assessment of Active Inflammation in Crohn Disease. Medicine. 2020;99(8):e19202. https://doi.org/10.1097/MD.0000000000019202
14. Yoshizako T, Wada A, Takahara T, Kwee TC, Nakamura M, Uchida K, et al. Diffusion-Weighted MRI for Evaluating Perianal Fistula Activity: Feasibility Study. European Journal of Radiology. 2012;81(9):2049–2053. https://doi.org/10.1016/j.ejrad.2011.06.052
15. Cavusoglu M, Duran S, Cılız DS, Tufan G, Çetin HH, Ozsoy A, et al. Added Value of Diffusion-Weighted Magnetic Resonance Imaging for the Diagnosis of Perianal Fistula. Diagnostic and Interventional Imaging. 2017;98(5):401–408. https://doi.org/10.1016/j.diii.2016.11.002
16. Hori M, Oto A, Orrin S, Suzuki K, Baron RL. Diffusion‐Weighted MRI: A New Tool for the Diagnosis of Fistula in ano. Journal of Magnetic Resonance Imaging. 2009;30(5):1021–1026. https://doi.org/10.1002/jmri.21934
17. Hilal SR, Hasan HS, Hasan AM. Magnetic Resonance Imaging Breast Scan Classification Based on Texture Features and Long Short-Term Memory Model. NeuroQuantology. 2021;19(7):41-47. https://doi.org/10.14704/nq.2021.19.7.NQ21082
18. Balcı S, Onur MR, Karaosmanoğlu AD, Karçaaltıncaba M, Akata D, Konan A, et al. MRI Evaluation of Anal and Perianal Diseases. Diagnostic and Interventional Radiology. 2019;25(1):21–27. https://doi.org/10.5152/dir.2018.17499
19. Hasan AM, Qasim AF, Jalab HA, Ibrahim RW. Breast Cancer MRI Classification Based on Fractional Entropy Image Enhancement and Deep Feature Extraction. Baghdad Science Journal. 2022;20(1):0221. https://doi.org/10.21123/bsj.2022.6782
20. Boruah DK, Hazarika K, Ahmed H, Borah KK, Borah S, Malakar S, et al. Role of Diffusion-Weighted Imaging in the Evaluation of Perianal Fistulae. Indian Journal of Radiology and Imaging. 2021;31(01):091–101. https://doi.org/10.1055/s-0041-1729673
21. Chao Gu, Yu Wang, Lixia Lai, Weiwei Han, Jiansheng Li, Haichang Xing, et al. A Comparable Method to Gdcontrast Enhancement in the Preoperative Evaluation of Anal Fistula. Medicine. 2019;98(44):e17807. https://doi.org/10.1097/MD.0000000000017807
22. Jean AA, Reddy AK, Elavarasi JA, Siddhartha N. Assessment of Role of Diffusion-Weighted Imaging in the Evaluation of Perianal Fistulae. International Journal of Academic Medicine and Pharmacy. 2023;5(3):461–464. http://dx.doi.org/10.47009/jamp.2023.5.3.99
23. Khera PS, Badawi HA, Afifi AH. MRI in Perianal Fistulae. Indian Journal of Radiology and Imaging. 2010;20(01):53–57. https://doi.org/10.4103/0971-3026.59756
24. Sharma A, Yadav P, Sahu M, Verma A. Current Imaging Techniques for Evaluation of Fistula in ano: a Review. Egyptian Journal of Radiology and Nuclear Medicine. 2020;51(1):1–18. https://doi.org/10.1186/s43055-020-00252-9
25. Mohsen LA, Osman NM. Diffusion-Weighted Imaging in the Evaluation of Perianal Fistula and Abscess. Egyptian Journal of Radiology and Nuclear Medicine. 2020;51:1–9. https://doi.org/10.1186/s43055-020-00193-3
26. Yoshizako T, Kitagaki H. A Pictorial Review of the Impact of Adding Diffusion-Weighted MR Imaging to Other MR Sequences for Assessment of Anal Fistulae. Japanese Journal of Radiology. 2013;31:371–376. https://doi.org/10.1007/s11604-013-0204-x
Noor Fadhil Baqir, BSc. (Radiological Engineering), College of Medical and Health Techniques, Middle Technical University, MRI technologist, Oncology Teaching Hospital in Medical City
Muasker, Al Rashid Street, Baghdad
Rasha Sabeeh Ahmed, BSc. (Physics), M.Sc. (Atomic Physics), Mustansiriyah University, Ph.D. (Nuclear Physics), Baghdad University, Professor at Physiology and Medical Physics Department, College of Medicine, Al-Nahrain University
Al-Jadria, Baghdad, 10072
Khaleel Ibraheem Mohsen, MD, Assistant Professor of the Radiology Department, Head of Clinical Department, National Cancer Research Center, University of Baghdad
Al-Jadria, Baghdad, 10072
Baqir N.F., Ahmed R.S., Mohsen Kh.I. Sensitivity of Diffusion-Weighted Image Combined with T2 Turbo Inversion Recovery Magnitude Sequence and as an Alternative to Contrast-Enhanced MRI in the Detection of Perianal Fistula. Advanced Engineering Research (Rostov-on-Don). 2023;23(3):307-316. https://doi.org/10.23947/2687-1653-2023-23-3-307-316



Advanced Engineering Research (Rostov-on-Don)
ISSN 2687-1653 (Online)
Contact with: Publisher / Editorial Office of the Journal
Publisher: Don State Technical University - DSTU, Rostov-on-Don, Russia - https://donstu.ru/en/
Editor-in-Chief: Alexey N. Beskopylny, Dr.Sci. (Eng.), Professor, Vice-Rector, Don State Technical University (Rostov-on-Don, Russia)
Don State Technical University
1, Gagarin Sq., Rostov-on-Don, 344003, Russia
tel.: +7 (863) 2738-372, e-mail: vestnik@donstu.ru
16+
Processing of personal data




































